In April 2012, Mental Health America of Greater Houston (MHA) launched the Harris County School Behavioral Health Initiative, a community-wide collaboration aimed at ensuring students with behavioral health needs are identified early and able to receive needed services. The initiative convened school district personnel, behavioral health providers, child-serving and education-related agencies, and parents to develop recommendations to improve the prevention, identification, and treatment of behavioral health issues among students. The initiative was born out of a 2003 report on school-based mental health care sites in Abilene, Austin, El Paso, Houston, Lubbock, Tarrant/Denton Counties, and Tyler. According to the report, counselors across the state faced challenges in providing appropriate levels of mental health services to students; teachers lacked both experience in recognizing early signs of mental health issues and an awareness of available community treatment resources; and schools burdened by financial constraints were unable to adequately meet the needs of students with mental health problems who were ineligible for services under federal law.
What began as a stakeholder meeting comprised of 40 organizations has grown into The Center for School Behavioral Health, thanks in large part to the ongoing commitment and engagement of collaborative members and generous philanthropic support. A major gift from the Houston Endowment enabled the creation of the Center, which serves as a “living laboratory” for incubating innovative, cost-effective and replicable best practices to improve the behavioral health of students by facilitating collective action; providing highly specialized professional development opportunities, technical assistance and community education; and conducting research, advocacy, and policy analysis. The long-term vision of the Center is to transform school behavioral health to support the healthy psychological and cognitive development of children in the Greater Houston region through services and programs promoting behavioral health, as well as the prevention, early identification, and treatment of behavioral health disorders.
School Behavioral Health Initiative: 37 Recommendations
Harris County School Behavioral Health Initiative (SBHI) meetings included personnel from ten school districts, county level educational organizations, behavioral health providers, child-serving agencies and advocacy organizations, and during the course of a year, workgroups prioritized the following activities:
- Review of state and federal laws that govern the identification and treatment of students with behavioral health issues, including the Individuals with Disabilities Education Act and Section 504 of the Rehabilitation Act, as well as relevant state regulations;
- Creation of a system “maps” of four school districts to determine their policies related to prevention, identification and treatment of mental health and/or substance use issues;
- Examination of national evidence-based and promising school behavioral health programs. These included best practices related to prevention, identification, and intervention;
- Completion of 32 individual interviews with key community members to obtain their views of how school behavioral health processes currently are working and ways in which they can be improved;
- Execution of site visits to locations that have been recognized statewide or nationally for innovative and best practice-based school mental health initiatives.
- Collection of data from the 20 Harris County school districts related to special education categorization, racial patterns, and disciplinary placements.
By February 2013, the SBHI developed and shared 37 recommendations based on their activities, including 7 recommendations for the Texas legislature:
- Restore the $5.4 billion in education funding cuts made during the 82nd Legislature
- Restore the almost $13 million in funding cuts made to Communities in Schools during the 82nd Legislature.
- Increase funding for substance use prevention, intervention and treatment for children and adolescents.
- Increase funding for children’s mental health treatment services.
- Designate at least 5% of current funding for children’s mental health treatment services to prevention programs, such as mental health literacy, personal safety, and suicide prevention.
- Appropriate General Revenue funds to increase grants for school-based health clinics.
- Require, in educator preparation programs, that teachers receive training in the detection of students with behavioral health issues.
Between 2013 and 2016, the School Behavioral Health Initiative worked toward system or district-wide implementation of the 37 recommendations. All seven of the legislative recommendations were fully or partially implemented, and 20 of the 21 school district recommendations were being implemented district-wide by at least one area school or charter school district. In total, 34 of the 37 recommendations have been realized.
85th Legislative Session Platform: Education
Guided by the 37 recommendations at the core of the Center’s advocacy efforts, MHA prioritized the development and implementation of school behavioral health services in our 85th Legislative Session Platform. Some may ask why it is necessary or, even, appropriate to address mental and behavioral health issues in a classroom environment instead of a home or doctor’s office. The answer to that question is simple, but not easy: One out of every five children has a mental illness or addictive disorder that causes some type of functional impairment. Youth with behavioral health issues may experience challenges such as academic underachievement, criminal justice involvement, and even suicide, and more than one-quarter of the total costs for mental health treatment services among adolescents were incurred in the education and juvenile justice systems. Lastly, children and adolescents spend much of their waking hours at school, making classrooms the ideal setting to recognize and initiate services to address the social, emotional and behavioral needs of our kids. Based on these facts, we support legislation focusing on school-based initiatives to improve prevention, identification and treatment of behavioral health issues among students. Specifically, we are looking at legislation related to behavioral health campus professionals, general reporting and trauma training, and transition services planning.
We spoke with Center for School Behavioral Health Director, Janet Pozmantier, and Professional Development Manager, Betsy Blanks, to get a comprehensive understanding of the legislative needs of the Center.
Janet: The Center came about because our schools were being overwhelmed with the number of children who were experiencing severe emotional difficulties and because of the severity of the difficulties our students were experiencing. We had long-time educators who were at a loss of what to do and how to handle so many children. We had a big win during the legislative session with Senate Bill 460, which mandates that all educators receive training in identifying the signs and symptoms of mental health problems among students and how to assist the child to get the appropriate help. We are grateful for that legislation being passed. It was very unusual because normally legislation does not pass right out the gate. Usually, it takes at least three sessions to pass.
What we have found four years later is that most of our educators are not aware of the fact that this mental health training is required, and the districts that are implementing the training do not have the time or resources to reach all of their teachers in an effective manner.
There are some wonderful evidence-based trainings out there. A free online training is Kognito At-Risk, a phenomenal interactive avatar based training. Unfortunately, free access to that may end and then I don’t know what’s going to happen. A lot of us offer the Youth Mental Health First Aid training. These trainings are free to districts through the Harris Center for Mental Health and IDD, our local mental health authority. However, there is a limit to how many the Harris Center can serve in any given year so organizations like Mental Health America of Greater Houston and NAMI are certified trainers. The challenge we have encountered is that our training is eight hours and costs money, limiting the number of school personnel who can take the training. The legislature did provide some money during the 83rd legislative session for these trainings but it is not enough to take care of the majority of teachers in the Greater Houston region because the money is to fund trainings statewide. That is a big problem.
The Center’s priority is getting these trainings out to people. Making sure people know about it. Currently, there are no “teeth” in the training legislation and that is why we have the proposed amendments to SB 460 that we are looking at today. There is no reporting requirement and so the schools are not going to do it. So, we want to make sure we have that reporting component inserted into the language of the updated bill. We also want to have trauma training included because of the things we have learned– especially from our conference this past fall — is there is an overwhelming desire from schools and districts to learn more about trauma and how it shows up in the classroom, and how to handle it. So many of the behavioral health problems we are seeing are not necessarily due to someone having a serious mental illness, but because it is a response to unresolved trauma and grief.
Betsy: Students who experience trauma are two and a half times more likely to be retained and are suspended and expelled more often. A student’s academic achievement can also be harmed because of trauma with reports of lower scores on standardized achievement tests and substantial impacts on IQ, reading achievement and language. Over the last ten years, teachers have really started to realize that this is an issue. Many of their students are not necessarily suffering from a mental illness but they are impacted by trauma. Teachers are recognizing it but they do not know what to do about it.
Annalee: Betsy, as a former teacher coming into this, what can you say about seeing both sides of this issue?
Betsy: The first time I attended the Mental Health First Aid course, it was after I started here at the Center, throughout the training, all day long, it just hit me over and over and over again how many kids I failed because I did not have this mental health training; the context. I worked at an inner-city school where kids were coming in with a lot of trauma and my school never talked about mental health, never talked about trauma. Teachers did not receive any information about that side of a child. It was all academic focus, and they did great things academically at my school, but you lose a lot of kids if you are not addressing that side. It was really hard as someone who cared deeply about being a good teacher and about my students. It was really difficult to later receive this training and get this information and look back and think about the specific children I let down because I was not prepared to handle their traumas. That’s not acceptable. We do such a disservice to our children in schools when our teachers are not prepared to address the whole child. They want to. No one goes into teaching with bad intentions. They want to do the best for their students and it’s not fair to the child to not equip our teachers with those tools. We send them to a lot of professional development and it’s not acceptable that at least a certain portion of that training is not dedicated to mental health training.
Janet: Our public schools are de facto providers of mental health services, and who is on the front lines at schools? The teachers. They don’t have the necessary training so we want to give them the tools to be trauma informed and understand mental health issues in order to understand how to refer out. We don’t want teachers to be therapists. That’s not their role. But who are they going to refer to? In many of our schools, there is no one there. Even if there is someone there, for example, school counselors are busying working on graduation plans and writing letters of recommendation or doing lunch line duties or testing. So, that is why we are advocating for one licensed behavioral health professional on every school. To help our teachers have more time to teach. If they identify a student who is in need of some type of service, then they can make sure that student gets those services. In other school districts around the country, schools have three, four, five counselors per grade because they realize a child cannot learn if they are experiencing homelessness, poverty, hunger, or trauma of any kind.
Trauma is everywhere, in all strata of society, and that is why we want a licensed behavioral health professional on every campus. I don’t buy the argument that we don’t have the money. We have the rainy-day fund, and you can get very creative with Medicaid reimbursement. We have great models here in Houston. Legacy Community Health has partnered with schools and figured out how to host integrated health care clinics on every campus so we can do this. You cannot live in a city like Houston and use the arguments that we cannot afford it. It’s not okay. Or in a state like Texas.
Behavioral Health Campus Professional
No conversation about improved prevention, identification and treatment of behavioral health issues among students would be complete without addressing the shortage of school counselors in Texas schools. National prevalence estimates indicate that one in five children have a mental illness or addictive disorder, meaning that approximately one million Texas public school students are dealing with these issues on a daily basis. These illnesses can cause mild to significant impairment in home and school activities and can lead to school failure, disciplinary placements, juvenile justice involvement, and, in extreme cases, suicide.
Despite the high prevalence of mental health and substance use disorders among children and adolescents, most schools do not have a designated staff person available to provide counseling or other needed services. In addition, school counselors, who historically were responsible for providing some of these services, are increasingly loaded down with administrative duties unrelated to mental or behavioral health counseling. They also are expected to handle increasingly large student caseloads.
Although the counselor shortage can be attributed to a mix of overburdened caseloads, funding cuts, and hiring shortages, the result is a student-to-counselor ratio well above the American School Counselor Association recommendation of 250-to-1. Following the 2011 cuts to public education, the Ray Marshall Center for the Study of Human Resources at the LBJ School of Public Affairs released Texas School Counselor Study: Exploring the Supply, Demand, and Evolving Roles of School Counselors. The study found “[b]eginning in 2012 and through 2014 the student-to-counselor ratio also remained relatively constant … between 460:1 and 470:1.” These numbers do not take into consideration the counselors’ ability to identify and address the behavioral health needs of students.

Credit: MARSHALL CENTER FOR THE STUDY OF HUMAN RESOURCES /UT AUSTIN

Credit: MARSHALL CENTER FOR THE STUDY OF HUMAN RESOURCES /UT AUSTIN
To address the shortage of counselors and other student support staff, MHA of Greater Houston supports legislation requiring at least one licensed behavioral health professional on each campus, as funding allows. While the long-term goal would be requiring one behavioral health professional per campus, the cost of associated with this type of legislation would be prohibitive in the current legislative climate. We have seen great success in meeting the behavioral health needs of students in public-private partnerships between school districts and community-based organizations like Communities in Schools and believe this is an incredibly positive starting point that would greatly benefit students.
Reporting and Trauma Training
MHA is incredibly proud of our work on Senate Bill (SB) 460, passed by the 83rd Texas Legislature in 2013. SB 460 requires school districts to provide teachers, administrators and staff with training in mental health intervention and suicide prevention to help them identify red flags in a child’s behavior and respond effectively. House Bill (HB) 2186, passed by the 84th Texas Legislature in 2015, requires suicide prevention training for all new school district and open-enrollment charter school educators annually and for existing school district and open-enrollment charter school educators on a schedule adopted by the Texas Education Agency (TEA) by rule.

Source: Understanding Child Trauma, National Child Traumatic Stress Initiative
Currently, Section 161.325 (Early Mental Health Intervention and Suicide Prevention), Health and Safety Code requires teachers, counselors, principals, and all other appropriate personnel to be trained in how to recognize and appropriately respond to signs of mental health and substance use disorders, as well as suicide. However, the trainings are not required to cover students who have experienced physical and emotional trauma. Additionally, there are not any reporting requirements to ensure that school districts are conducting the trainings.
The goal of MHA’s proposed general reporting and trauma training legislation is two-fold: 1) to provide accountability measures to reinforce the training mandate through reporting to the Texas Education Agency; 2) to require all school personnel to receive training in how to recognize and appropriately respond to signs of trauma.
As proposed, this legislation would amend SB 460 to require school districts to train educators in how to recognize and appropriately respond to physical and emotional trauma, as well as to report all training information to the Texas Education Agency. This accountability measure does not serve as a new mandate. SB 460 already requires school district employees to receive training. The school district is also required to keep records of all training participation. This amendment would strengthen the already existing requirements in the bill by ensuring the records kept by the district on the required training would then be reported to the TEA and be accessible to parents and community members.
To better understand the need for trauma training and the impact of trauma on students, Annalee Gulley sat down with Julie B. Kaplow, Ph.D., A.B.P.P., Director of the Trauma and Grief Center for Youth at The University of Texas Health Science Center at Houston. The Trauma and Grief Center for Youth opened in December 2014 and treats youth ages seven to 17 who have experienced trauma and loss.
Annalee: If you were a teacher and were in your classroom, what are some of the signs you might recognize in a child who has experienced some type of trauma?
Julie: What makes this difficult is that posttraumatic stress symptoms can look a lot like ADHD symptoms. We will often hear from teachers, “This child won’t sit still. They are distracted. They seem like they are in another world. You say one thing that sets them off and you cannot seem to calm them down.” These may be signs of ADHD, but they can also be signs of posttraumatic stress. It is important to help teachers understand how kids may react in the aftermath of trauma and put these behaviors into context. Many traumatized kids may be triggered without knowing why inside the classroom. It is often helpful to inform teachers about potential trauma reminders – people, places, situations, or things that remind kids of the frightening thing that happened to them. Trauma reminders can be as subtle as kids screaming on the playground (if the traumatic event involved the sound of screams) or the teacher giving that child a certain look or scolding them. These kids often get mislabeled or are misunderstood as “behavior problems” when in fact they are simply reacting to their environment and are being reminded of whatever traumatic experience they had.
A trauma training would help to educate teachers about the many ways in which various forms of trauma and adverse life events, such as the death of a loved one, as well as accompanying posttraumatic stress or maladaptive grief can impact learning and how this may manifest in the classroom. When teachers really do understand how trauma impacts children, they are able to have more empathy in the classroom, they are better able to see why certain children may be behaving the way they are and are then able to help them to modify those behaviors in a much more effective way. What we also know is that teachers can use all of the behavioral strategies and positive reinforcement they want with a traumatized child, but if they are not able to identify what it is that is triggering them, that’s not going to help them in the classroom. A trauma training for teachers would help to explicate the ways in which posttraumatic stress and/or grief reactions can manifest in the classroom and what teachers can do to help these youth to de-escalate and stay on track.
Annalee: How would you respond to the argument that this is not a teacher’s job? That we are turning teachers into counselors or behavioral health professionals when we ask them to identify a child who has been traumatized or ask them to de-escalate a situation or determine whether a child has been abused or is suffering PTSD?
Julie: I would say that, first, we are obviously not asking teachers to treat a child’s posttraumatic stress because that would require a higher level of training and intervention. What we are suggesting though is that teachers can play a critical role in identifying those youth who may need to be referred for an evaluation. It is important to remember that, for many traumatized youth, their teachers may be the only adults in their lives who are actually seeing their posttraumatic reactions and/or behaviors. So the school can actually serve as a critical point of entry. In addition, we know that trauma and PTSD can directly impede the child’s ability to learn, and a primary goal of most teachers is to create an environment in which all kids in the classroom are able to learn in the most effective way possible. When youth are struggling with PTSD, this may directly interfere with the primary goal for teachers. By empowering teachers with the knowledge and information needed to identify trauma and PTSD in youth, they will begin to feel like they have more control over their classroom. We see many teachers, particularly in underserved communities, who are faced with a lack of resources and high levels of trauma in the neighborhoods in which they work. Many teachers feel overwhelmed and think “I’ve just got to get through this day” as opposed to ” I am starting to notice a pattern with this child and this might be a sign that they have a history or trauma.” This new knowledge allows teachers to feel more in control of their classroom, less overwhelmed, and better equipped to refer those kids who may need a thorough trauma-informed evaluation and/or intervention.
Transition Services Plan
To ensure students with prolonged placements in out-of-school facilities, including disciplinary programs and residential treatment facilities to address disciplinary or behavioral health needs, have a continuum of services, MHA of Greater Houston seeks to require the creation of a transition plan for the returning student. Annalee Gulley spoke to Latashia Crenshaw, Director of Educational Support and Advocacy Services at the Harris County Juvenile Probation Department. The Education Support and Advocacy Services is tasked with “advocate[ing] for improved educational services for probation-involved youth in community settings.”
Annalee: When you are able to get them back to the home campus, do you encounter many schools that have the ability or systems in place to integrate that child successfully back into school?
Latashia: Some districts, as with everything, are better than others when it comes to transitioning our youth back into their home school. It also depends on how long the youth has been out of their system and involved in our system. For youth who have not been out of their home school for very long, I can say that they have much easier chances transitioning back into the school from an out-of-school facility. Those who have been out of their school for quite a while, or not attending their home school prior to coming to us, those are the youth who concern us the most. We are trying to focus on making sure we have the correct records, the correct grade level for that student or making sure that the special education services are in place. Transitioning the services we have in place while the youth are in a placement because they may look completely different than what needs to happen when the youth returns to the home school. We have found there are gaps when making sure there is a continuum of support and services between placements.
Annalee: If you were to help facilitate the process of creating a standardized transition plan, what do you think some of the core elements of the plan would need to include?
Latashia: In an ideal world, we would have transition specialists or people designated in the district who would track youth who have been withdrawn from their district and in our facility because once the youth is enrolled in our system for a designated number of days, they are withdrawn from their home district and placed in our school system.
For transition plans, if the youth is in our facility — for say 60 days or longer– if we could have a transition specialist work with us when we know that youth is going to be released, to have the home school become involved with the youth transition plan so that we can ensure that everything is in place when they go back to the home school. This would include setting up Admission, Review, and Dismissal (ARD) meetings, as well as 504 meetings because most of our students have some sort of disability. A transition plan would definitely include looking at the courses the youth is enrolled in with us versus what they need to be enrolled in when they return to their home school. Again, what types of transition services this youth would need just to really get reintegrated back into their home school system versus the education system we were involved in. To me, a transition plan would include reintegration meetings prior to the youth being released, including staff from probation, the home school and any other services they are going to be involved with in the community. Some sort of meeting that includes all the people who are going to be working with the student and family.
Latashia: I cannot stress how significant it would be, especially for those youths who have significant mental health concerns and disability, to collaborate on transition meetings while the youth is in placement. This would include having home school personnel come to ARD meetings or hold these meetings in conjunction with our staff so that we can ensure that when this youth leaves placement they are actually successful with transitioning back to their home school and don’t return to us simply because records are not there or they are sitting at home waiting to be in enrolled in a school, which may or may not happen.
What’s Next?
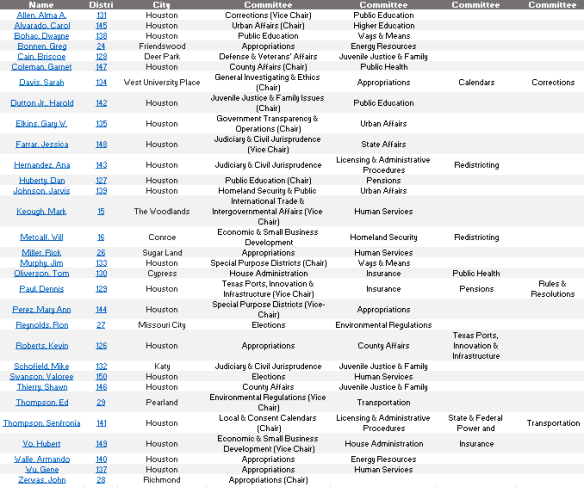
As we build support for this legislation in Austin, we will report on important milestones like bill filings, committee assignments, and committee hearings. Your voices need to be heard by legislators to ensure they understand the importance of these issues for students in Houston and beyond. Stay tuned!